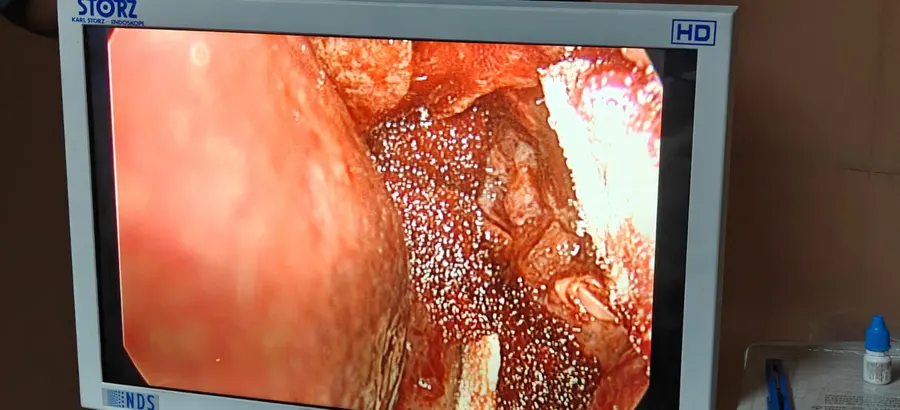
⭐ Endoscopic DCR (Karl Storz) | Nasal route, no external incision, no scar. Performed in collaboration with Dr. Vibhor Malhotra, Consultant ENT Surgeon. Karl Storz high-definition endoscopic system. |
DCT (Dacryocystectomy) | Removal of the lacrimal sac when DCR is not suitable. Eliminates recurrent dacryocystitis. |
DCR (Conventional External) | Traditional skin incision approach with creation of new ostium. Long-established technique with excellent outcomes. |
DCR with Intubation | Silicone tube intubation of the lacrimal system during DCR for cases with narrow canaliculi or revision surgery. |
Sac Syringing with Antibiotics | Diagnostic and therapeutic irrigation of the lacrimal system. One or both sides. First-line assessment for watering eyes. |
Punctal Plug — Temporary (Single Punctum) | Dissolvable plug in one tear drainage opening of a single eye. For trial of punctal occlusion. |
Punctal Plug — Temporary (Both Puncta) | Dissolvable plugs in both upper and lower puncta of a single eye for comprehensive tear conservation. |
Punctal Plug with Antibiotic Irrigation | Combined punctal plug insertion with antibiotic lavage. Both puncta of a single eye. |
Punctal Plug — Permanent (Dry Eye) | Silicone plug permanently placed for aqueous-deficient dry eye. Long-term tear conservation. |
Punctal Cautery | Permanent cauterisation of the punctal opening for severe dry eye where plugs are insufficient. |
Ptosis Repair — Suture Sling | For ptosis with fair levator function. Frontalis suspension using prolene suture. |
Ptosis Repair — Silicone Sling | For ptosis with poor levator function. Silicone rod suspension to frontalis muscle. |
Entropion Repair | Lid-tightening procedure to correct inward-turning eyelid margin. |
Ectropion Repair | Lid-tightening or repositioning procedure to correct outward-turning eyelid margin. |
Chalazion I&C | Incision and curettage of eyelid meibomian gland cyst under local anaesthesia. |
Lid Mass Removal | Excision of benign or suspicious eyelid lesion with primary closure or reconstruction. |
Lid Repair — Minor | Repair of minor eyelid laceration not involving the lid margin or lacrimal system. |
Lid Repair — Major | Repair of major lid trauma including lid margin, canaliculus, or significant tissue loss. |
Evisceration | Removal of intraocular contents preserving the scleral shell. For blind, painful eye. |
Enucleation | Removal of the entire globe. For blind painful eye, intraocular tumour, or trauma. |